

Cataract and Cataract - Refractive Surgery
Cataracts occur when the natural lens of the eye becomes cloudy, causing vision impairment. Cataract surgery is one of the most common and successful procedures performed to restore clear vision.
Cataract and Cataract - Refractive Surgery
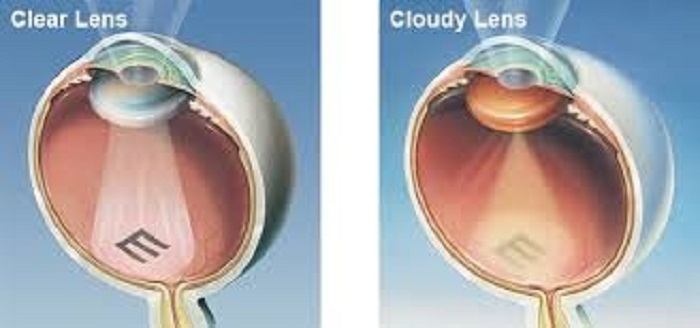
Eyes have an important structure called lens, which helps focus the rays of light on to the retina. Clouding or opacification of the lens is cataract.
This may be present at birth or occur due to injury but the most common variety is related to age (Senile Cataract). This is the most common cause of visual disability in the aged population.
Cataract is the Commonest Cause
Cataract is the commonest cause of preventable blindness in the world. The treatment is surgical with replacement of the opacified lens with an artificial intraocular lens.
The current method of performing suture less surgery with a small incision by using the phacoemulsification machine and the introduction of a foldable lens results in early visual rehabilitation.
Centre for Eye and Health Care (CEHC) is equipped with the latest microscopes and phacoemulsification machines and the surgeries are done in modern operating theatres with standards as defined by NABH and with disposable consumables from companies of repute for optimal results.
The options of cataract removal are, manual or by phacoemulsification.
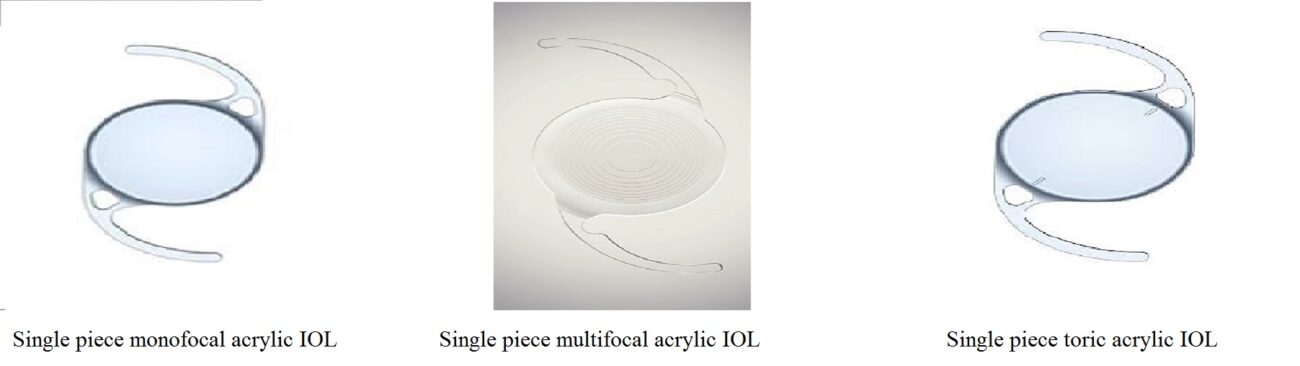
Intraocular lens(IOL).
IOL and The techniques
The type of IOL and the techniques to be adopted depends on the eye condition, type of cataract, cost and requirement of the patient. It is best to discuss with your surgeon and decide on the type of lens suited for you.
